control of sub clinical ketosis
Subclinical Ketosis. Economic Implications and Clinical Management
Published: October 1, 2012
By: Dr. Henna Hamadani, Division of Livestock Production & Management,Sher e Kashmir University of Agricultural Sciences & Technology,Kashmir, India -190006
INTRODUCTION
Subclinical ketosis (SCK) is defined as elevated concentrations of ketone bodies in the absence of clinical signs of ketosis. It is an important metabolic disease in dairy cattle during early lactation period and has been associated with decreased milk production, impaired reproductive performance, displaced abomasums, metritis, mastitis, and clinical ketosis (Duffield,2001). During the early postpartum period, milk production increases dramatically, while energy intake may not be adequate to sustain the higher production level. This results in negative energy balance and cows metabolize body fat to meet their energy needs, resulting in increased production of ketone bodies in liver when gluconeogenic precursors are limiting. About 40% of dairy cows suffer post partum from subclinical ketosis and 5% of affected cows are culled. Without treatment, the case-fatality rate approaches 100%. Since the disease goes unnoticed because of the absence of clinical signs, treatment is delayed while the performance of the animals is getting affected, hence causing heavy economic losses. Subclinical ketosis costs are estimated at $78 per case; therefore, based on 40% prevalence in a 100-cow herd, the economic loss is approximately $3,120 per year (Geishauser et al., 2001).
It occurs mostly in high yielding milking animals. Cows, ewes and she- buffaloes mostly suffer from this condition. Pregnancy toxaemia in ewe has got identical biochemical pathways though there are differences in clinical signs. Indigenous cattle seldom suffer from this problem. High yielding cattle generally suffer either within a month after calving or any time during lactation period. This is because all high yielding cows in the early lactation remain in negative energy balance. Infrequently it can be observed in dry cows which are in late pregnancy.
INCIDENCE
The incidence of ketosis is higher in third lactation or following that. Subclinical ketosis occur more commonly than clinical ketosis and have significant economic importance. It is estimated that the incidence of subclinical ketosis during the first three weeks of lactation averages 30% in most herds. A significant relation between animal age, number of parturition, mastitis and subclinical ketosis have been reported by Dohoo et al. (1984). Subclinical ketosis was more likely to be found in cows experiencing metritis than in unaffected cows (Dohoo and Martin,1983).Various studies have shown that subclinical ketosis is common in high producing cows 2-7 weeks post partum, with recorded prevalence ranging from 7-34%. It has been reported that peak incidence of SCK occurred at 5 days in milk (DIM), when 22.3% of cows had their first SCK-positive test. Whereas peak prevalence of SCK occurred at 5 DIM, when 28.9% of cows had a SCK-positive test (McArt et al.,2012). In a study carried out in Dairy Cows in Fars Province of Iran by Marjan and Saman (2011), the incidence rate of subclinical ketosis was 7.2% (percent of cows with at least one positive test) in early lactation (0-70th day) period and the peak prevalence of subclinical ketosis occurred during the fourth week of lactation.
CLINICAL FINDINGS
In early lactation there are likely to be many dairy cows in which marked indications of carbohydrate insufficiency and fat mobilization can be detected, but which do not exhibit any clinical signs of ketosis. When these indications include hyperketonemia and hypoglycemia, the cows may be considered to be suffering from subclinical ketosis (Schwalm and Schultz,1976). that the condition may remain undetected and, hence, untreated, and yet have adverse effects
on productivity which parallel those elicited by clinical ketosis. In subclinical ketosis, urine and blood contain ketone bodies in excess amounts without showing obvious symptoms of ketosis but will have diminished productivity including depression of milk yield and a reduction in fertility. Potential milk production is reduced by 1 – 9 %. Surveys of large populations show a declining prevalence of ketosis positive cows after a peak in the period immediately after calving, and a positive relationship between hyperketonemia and high milk yield. Infertility may appear as an ovarian abnormality, delayed onset of estrus or as endometritis resulting in an increase in calving to conception interval and reduced conception rate at first insemination. In Europe, endometritis itself is thought to be a sequel to a nutritional stress at this time, but much of the sress there is due to overfeeding in early lactation which increases the risk for both endometritis and acetonemia.
CLINICAL PATHOLOGY
Hypoglycaemia, ketonaemia and ketonuria are characteristics of the disease. There is an increase in plasma free fatty acids in some cases.
A) Blood Sugar Level
In normal animals the blood sugar level is 40mg/100 ml of blood where as in ketotic animal it is reduced.
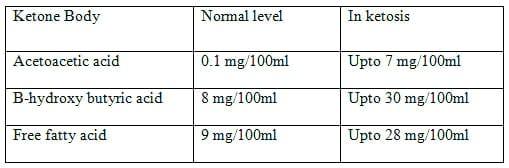
B) Ketone Bodies Level
1. In Blood:
The ketone body level increases in the blood of the ketotic cows as shown in the table below:
2. In Milk:
Ketone bodies are not exreated in milk normally but in ketosis, ketone bodies are exreated at the rate of 40mg/100ml milk. Sweet odour of ketone bodies can be also detected in milk.
3. In Urine:
Ketone bodies are not exreated in urine normally but in ketosis, upto 500-1000mg ketone bodies /100ml of urine are exreated.
Biochemical Test For Detection Of Ketone Bodies In Urine (Modified Rothera’s Test)
A mixture produced by the reagents (100g Ammonium sulphate, 50g Anhydrous sodium sulphate and 3g Sodium nitropruside) is taken upto half of a test tube, the suspected urine is slowly added through the wall of the test tube to form a layer on the top of the reagent. Without mixing, the test tube is set aside for a few minutes. In positive cases, KMnO4 colour quickly appears. In field conditions milk can be used instead of urine.
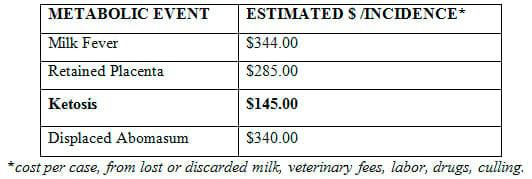
ECONOMIC IMPLICATIONS
In cattle:
Clinical and subclinical ketosis is one of the major causes of the major causes of loss to the dairy farmer. Sub-clinical ketosis is however far more costly than clinical ketosis which is visible and treated; as will bring on immune deficiency symptoms mostly commonly verified in elevated cell count and clinical mastitis. In rare instances the disease is irreversible and the affected animal dies but the main economic loss is due to the loss of production while the disease is present and failure to return to full production after recovery. Both clinical and subclinical ketosis are accompanied by decreased milk yields and lower milk protein and milk lactose and increased risk for delayed estrus and lower first service conception rates, increased intercalving intervals and increased risk of cystic ovarian disease and mastitis.
In sheep:
The economic effect of the disease is considerable. Without treatment, the case-fatality rate approaches 100% and individual flocks the disease can reach a level of incidence sufficient to be classed as an outbreak. Flocks that experience pregnancy toxaemia will also have a higher than normal mortality in neonatal lambs and usually a decrease in wool quality. Pregnanacy toxaemia predisposes to hypomagnesemia in sheep.
MANAGEMENT:
Herd level management:
Suggested Protocols:
- For dry cow and transition periods:
Check 12 cows within the first two weeks of freshening. If 2 or more cows are positive, consult with your veterinarian and/or nutritionist to evaluate herd management practices during the dry cow and transition periods.
- For herd health and nutrition management:
Check 12 cows in each feeding group quarterly. If 2 or more cows test positive, consult with your nutritionist to evaluate herd feed rations.
Individual cow management:
Cows should be monitored for BHB at 2 to 14 days in milk when the incidence of subclinical ketosis peaks. In some cases, this period may extend to 21 days.
- Recommended Protocol: Test all fresh cows once a week during the first two weeks of lactation (identifies approximately 95% of subclinical cows).
- Alternate protocols:
• Test fresh cows once during the second week of lactation (identifies approximately 69% – 86% of subclinical cows).
• Test fresh cows once during the first week of lactation (identifies approximately 30% – 56% of subclinical cows).
• Test fresh older cows (second or greater lactation).
• Test fresh cows with body condition score > 4.
• Test fresh cows during periods of heat stress.
CLINICAL MANAGEMENT
- Adopt modified Rothera’s test or ketostick test routinely on milk or urine.
- Use propylene glycol as a preventive package in positive cases.
- Use glucose; propylene glycol along with glucose will be a better package.
- Use long acting glucocorticoid which will keep the glucose level for a long period.
- If it does not work use insulin as a supportive therapy.
LINE OF TREATMENT:
1. Replacement therapy:
The only rational treatment in ketosis is to relieve the need for glucose formation from tissues and allow ketone body utilization to continue normally. Theoretically the simplest means of doing so is this by the administration of glucose replacement therapy. Generally 500 to 800 c.c. of a 40-50% solution of glucose ( Dextrose solution) should be administered intravenously at once. To overcome the necessity of repeated injections oral hyperglycemic agents should be given which maintain glucose level in blood.
Oral Hyperglycemic Agents (Glucose Precursors)
A) Glycerol or Glycerine (medicated or purified glycerine)
Dose: Adult cattle : 100 mg twice daily for 2 or 3 days.
Small cattle : 50 mg twice daily for 2 or 3 days.
B) Instead of glycerine, propylene glycol may be used.
Dose : More or less 2 folds of glycerine, but is not always available.
C) Sodium propionate: Because of glucogenic effect of propionate, it can be given at the dose of 100 – 200 g once daily for 3 days to cattle.
D) Lactates are also highly glucogenic. Na-lactate and Ca-lactate are used.
Dose: 1 kg initially followed by 0.5 kg daily for 7 days as maintenance dose.
E) Sodium acetate 110-500 gm daily orally gives less satisfactory results.
2. Hormonal Therapy
Injection with adrenals corticoids is modern treatment which is dramatically successful in field cases.
a) Betamethasone and dexamethasone are very much effective and can be given upto 30mg I/M. one injection may be sufficient but a second may be necessary in some cases.
b) Triamcinolone (Vetalog) is very much active against ketosis. Generally it is available in 1 ml vial. Glucocorticoid reduces ketone body formation by utilization of Acetyl CoA and raising blood glucose level by making greater availability of glucose precursor in the liver.
Dose:
Small Animal : 1 ml I/M
Large Animal : 5 ml I/M
c) Prednisolone (Hostacortin-H) – can also be employed in ketosis. Available in 10 ml vial (1000mg) 1 ml solution contain 10 mg og prednisolone.
Dose:
Large animal : 10 ml
Small animal : 5 ml
3. Insulin therapy
Generally protamine zinc is used Dose : 200 I.U. for large animals. Sometimes insulin and glucosteroids can be administered simultaneously. This is known as combination therapy or simultaneous therapy. Dose: 200 I.U. of insulin and 10 mg dexamethasone. Insulin is powerful antiketogenic & suppressor of NEFA mobilization.
4. MISCELLENEOUS TREATMENT:
a) Choral hydrate: an initial dose of 30 g can be followed by 7 g doses twice daily twice for 3-5 days
b) Vit. B12 and cobalt.
c) Cysteamine and sodium fumerate have also been used.
d) Lipotropic substances:
Methionine @ 200 g in 500 ml of water I/V
Choline @ 25 g in 500 ml of water orally
Supportive : Inj. Liver extract @ 5-10 ml alternate day for 3 injections
CONTROL
Existing evidence favors the concept that the most successful control of the ketosis problem through feeding and management could be obtained by :
1) Providing feeds containing adequate nutrients according to current feeding standards.
2) Offering these feeds at levels as near optimum as possible within the ability of the cow to consume them without going off feed.
3) Following management practices which maximize intake in early lactation and minimize prolonged mobilization of body fat as well as intake of ketogenic materials.
PREVENTION:
Although there is no known preventive procedure which would guarantee freedom from ketosis, the following specific suggestions are made:
1) Avoid excessive fatness at calving.
2) Increase concentrate feeding to moderate levels in the late dry period and rapidly after calving, using care to prevent the cow from going off feed.
3) Feed high-quality roughage at a minimum one-third of total dry matter intake. Do not make abrupt changes in the ration, particularly to low-quality materials. 5) Feed recommended protein, minerals, and vitamins.
4) Avoid hay crop silage high in butyric acid.
5) Maximize intake by providing for adequate comfort, exercise, and absence of stress.
6) In problem herds, monitor the ketotic state by weekly milk tests, and feed propylene glycol to susceptible cows.
7) Production being equal, select strong cows with good appetites.
REFERENCES
Dohoo, I. R., Martin, S.W., McMillian, I., Kennedy, B.W.,1984. Disease production and culling in Holstein - Friesian cow. II age, season and sire effect. Preventive Veterinary Medicine. (2) 665-671.
Dohoo, I.R. and Martin, S.W. 1983.Subclinical Ketosis: Prevalence and Associations with Production and Disease. Canadian Journal of Comparative Medicine. 48: 1-5.
Duffield, T. 2001. Importance of Subclinical Ketosis in Lactating Dairy Cattle. Procedings of Michigan Veterinary Conference.
Geishauser, T., K. Leslie, D. Kelton, and T. Duffield. 2001. Monitoring for subclinical ketosis in dairy herds. Compendium, Food Animal. 23(8):S65-S71.
Marjan, H.J. and Saman, N.,2011. Incidence of Subclinical Ketosis in Dairy Cows in Fars Province of Iran and Reproductive Performance in Early Lactetion Period. Asian Journal of Animal Sciences. 5 (2): 158-161
McArt, J.A.A., Nydam, D.V. and Oetzel, G.R., 2012. Epidemiology of subclinical ketosis in early lactation dairy cattle. Journal of Dairy Science. 95(9): 5056-5066
Schwalm, J. W., and L. H. Schultz. 1976. Relationship of insulin concentration to blood metabolites in the dairy cow. Journal of Diary Science. 59:255.
Related topics:
Authors:


Recommend
Comment
Share
26 de septiembre de 2020
Informative Article. Ketosis is a metabolic disease that occurs when the cow is in a severe state of negative energy balance. This condition arises from disturbances in the metabolism of carbohydrates and volatile fatty acids in the body.
Recommend
Reply
16 de octubre de 2012
I think it is imposible over feeding in dairy animal at early lactation but at the end period of pregnancy. Thank you, Ferdinal Rahim
Recommend
Reply

13 de octubre de 2012
best supportiv information about ketosis for veterinarian and also for dairy farmers.
Recommend
Reply

11 de octubre de 2012
It is very deep and interesting solution for dairy farmers and professionals.
Recommend
Reply

Would you like to discuss another topic? Create a new post to engage with experts in the community.






Featured users in Dairy Cattle




José Manuel Oropeza Meza
MSD - Merck Animal Health
Gerente Nacional Cuentas Clave en MSD Salud Animal
United States
United States