Calcium, vitamins and phosporus in poultry diets
Metabolic Bone Disorder: Rickets
Published: October 19, 2011
By: Dr. S. F. Nipane and Dr. A. N. Panchbuddhe (Suman Hatchery Ltd.)
Rickets can occur in young birds due to insufficient Vitamin D3, calcium and/or phosphorus. Commercial feeds and supplements provide these nutrients, but if they are over-diluted, the birds will not get enough.
Birds can synthesize their own Vitamin D, to a certain extent, with exposure to sunlight. A deficiency of any of these nutrients can also lead to problems with egg-laying birds. Egg production may be reduced and/or the quality of the egg shell may be poor. In severe cases hens may be afflicted with a disease called cage-layer fatigue (brittle-bone disease, osteoporosis).
Metabolic Bone Disorders/Diseases:
Causes of Leg Problems:
Non-infectious:
- Rickets
- Osteoporosis
- Osteopenia
- Curled toe paralysis
- Perosis or slipped tendon
- Tibial Dyschonlasia
- Angular Bone Deformity
- Crooked Toes
- Spondylolisthesis
- Scoliosis
- Osteomylitis
- Rotated tibia/Twisted leg/Valgus and Varus deviations of tibiotarsi (VVD)
Infectious:
- Femoral Head Necrosis
- Chondrodystrophy
- Bacterial Synovitis
- Arthritis
- Osteomyelitis
- Viral Arthritis
- Synovitis
Species:
Rickets and nutritionally based bone problems occur in chicken, turkey and duck and specialty types of birds. All birds, particularly fast growing birds fed "home formulated" diets may be affected.
Body Distribution of Calcium and Phosphate
There are three major pools of calcium in the body:
- Intracellular calcium: A large majority of calcium within cells is sequestered in mitochondria and endoplasmic reticulum. Intracellular free calcium concentrations fluctuate greatly, from roughly 100 nM to greater than 1 uM, due to release from cellular stores or influx from extracellular fluid. These fluctuations are integral to calcium´s role in intracellular signaling, enzyme activation and muscle contractions.
- Calcium in blood and extracellular fluid: Roughly half of the calcium in blood is bound to proteins. The concentration of ionized calcium in this compartment is normally almost invariant at approximately 1 mM, or 10,000 times the basal concentration of free calcium within cells. Also, the concentration of phosphorus in blood is essentially identical to that of calcium.
- Bone calcium: A vast majority of body calcium is in bone. Within bone, 99% of the calcium is tied up in the mineral phase, but the remaining 1% is in a pool that can rapidly exchange with extracellular calcium.
As with calcium, the majority of body phosphate (approximately 85%) is present in the mineral phase of bone. The remainder of body phosphate is present in a variety of inorganic and organic compounds distributed within both intracellular and extracellular compartments. Normal blood concentrations of phosphate are very similar to calcium.
Fluxes of Calcium and Phosphorus
Maintaining constant concentrations of calcium in blood requires frequent adjustments, which can be described as fluxes of calcium between blood and other body compartments. Three organs participate in supplying calcium to blood and removing it from blood when necessary:
- The small intestine is the site where dietary calcium is absorbed. Importantly, efficient absorption of calcium in the small intestine is dependent on expression of a calcium-binding protein in epithelial cells.
- Bone serves as a vast reservoir of calcium. Stimulating net resorption of bone mineral releases calcium and phosphate into blood, and suppressing this effect allows calcium to be deposited in bone.
- The kidney is critically important in calcium homeostasis. Under normal blood calcium concentrations, almost all of the calcium that enters glomerular filtrate is reabsorbed from the tubular system back into blood, which preserves blood calcium levels. If tubular reabsorption of calcium decreases, calcium is lost by excretion into urine.
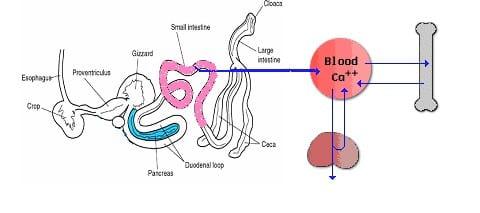
Fig1: Fluxes of Calcium
Hormonal Control Systems:
Maintaining normal blood calcium and phosphorus concentrations is managed through the concerted action of three hormones that control fluxes of calcium in and out of blood and extracellular fluid:
Parathyroid hormone serves to increase blood concentrations of calcium. Mechanistically, parathyroid hormone preserves blood calcium by several major effects:
• Stimulates production of the biologically-active form of vitamin D within the kidney.
• Facilitates mobilization of calcium and phosphate from bone. To prevent detrimental increases in phosphate, parathyroid hormone also has a potent effect on the kidney to eliminate phosphate (phosphaturic effect).
• Maximizes tubular reabsorption of calcium within the kidney. This activity results in minimal losses of calcium in urine.
Vitamin D acts also to increase blood concentrations of calcium. It is generated through the activity of parathyroid hormone within the kidney. Far and away the most important effect of vitamin D is to facilitate absorption of calcium from the small intestine. In concert with parathyroid hormone, vitamin D also enhances fluxes of calcium out of bone.
Calcitonin is a hormone that functions to reduce blood calcium levels. It is secreted in response to hypercalcemia and has at least two effects:
• Suppression of renal tubular reabsorption of calcium. In other words, calcitonin enhances excretion of calcium into urine.
• Inhibition of bone resorption, which would minimize fluxes of calcium from bone into blood.
Although calcitonin has significant calcium-lowing effects in some species, it appears to have a minimal influence on blood calcium levels.
Maintaining normal blood calcium and phosphorus concentrations is managed through the concerted action of three hormones that control fluxes of calcium in and out of blood and extracellular fluid:
Parathyroid hormone serves to increase blood concentrations of calcium. Mechanistically, parathyroid hormone preserves blood calcium by several major effects:
• Stimulates production of the biologically-active form of vitamin D within the kidney.
• Facilitates mobilization of calcium and phosphate from bone. To prevent detrimental increases in phosphate, parathyroid hormone also has a potent effect on the kidney to eliminate phosphate (phosphaturic effect).
• Maximizes tubular reabsorption of calcium within the kidney. This activity results in minimal losses of calcium in urine.
Vitamin D acts also to increase blood concentrations of calcium. It is generated through the activity of parathyroid hormone within the kidney. Far and away the most important effect of vitamin D is to facilitate absorption of calcium from the small intestine. In concert with parathyroid hormone, vitamin D also enhances fluxes of calcium out of bone.
Calcitonin is a hormone that functions to reduce blood calcium levels. It is secreted in response to hypercalcemia and has at least two effects:
• Suppression of renal tubular reabsorption of calcium. In other words, calcitonin enhances excretion of calcium into urine.
• Inhibition of bone resorption, which would minimize fluxes of calcium from bone into blood.
Although calcitonin has significant calcium-lowing effects in some species, it appears to have a minimal influence on blood calcium levels.
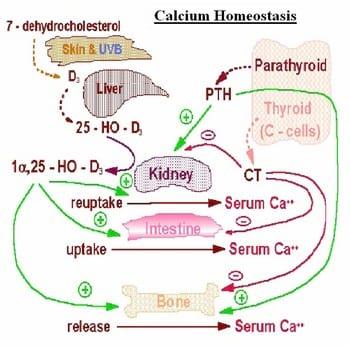
Fig 2: Endocrine Control of Calcium Homeostasis
A useful way of hormones affect tissues to preserve calcium homeostasis is to examine the effects of calcium deprivation and calcium loading.
The following table summarizes body responses to conditions that would otherwise lead to serious imbalances in calcium and phosphate levels in blood.
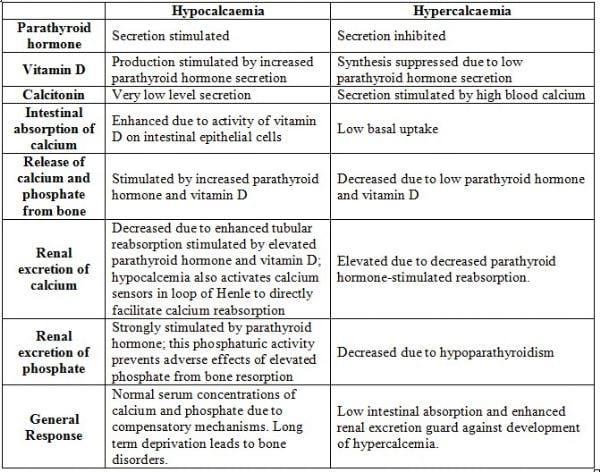
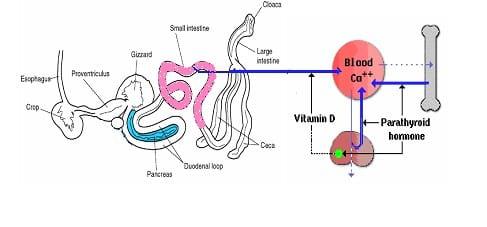
Fig 3: Calcium Deprivation
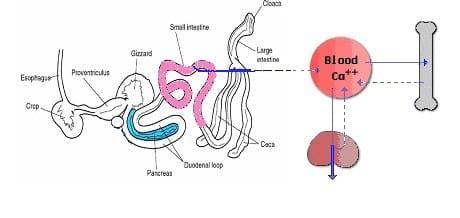
Fig 4: Calcium Loading
Structure and Synthesis:
The term Vitamin D is, unfortunately, an imprecise term referring to one or more members of a group of steroid molecules. Vitamin D3, also known as cholecalciferol is generated in the skin of animals when light energy is absorbed by a precursor molecule 7-dehydrocholesterol.
Vitamin D is thus not a true vitamin, because individuals with adequate exposure to sunlight do not require dietary supplementation. There are dietary sources of Vitamin D, including egg yolk, fish oil and a number of plants.
The plant form of Vitamin D is called Vitamin D2 or ergosterol. However, natural diets typically do not contain adequate quantities of Vitamin D, and exposure to sunlight or consumption of foodstuffs purposefully supplemented with Vitamin D are necessary to prevent deficiencies
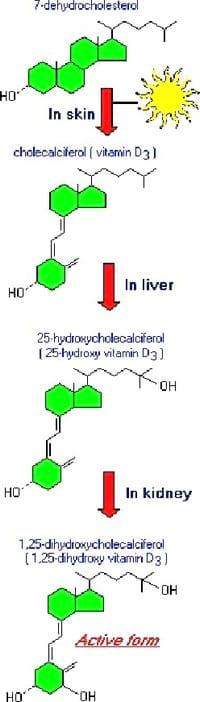
Fig 5: Pathway of synthesis of Vitamin D3
Vitamin D, as either D3 or D2, does not have significant biological activity. Rather, it must be metabolized within the body to the hormonally-active form known as 1,25-dihydroxycholecalciferol. This transformation occurs in two steps, as depicted in the diagram to the right:
- Within the liver, cholecalciferal is hydroxylated to 25-hydroxycholecalciferol by the enzyme 25-hydroxylase.
- Within the kidney, 25-hydroxycholecalciferol serves as a substrate for 1-alpha-hydroxylase, yielding 1,25-dihydroxycholecalciferol, the biologically active form.
Each of the forms of Vitamin D is hyhobic, and is transported in blood bound to carrier proteins. The major carrier is called, appropriately, Vitamin D-binding protein. The halflife of 25-hydroxycholecalciferol is several weeks, while that of 1,25-dihydroxycholecalciferol is only a few hours.
Physiological Effects of Vitamin D:
Vitamin D is well known as a hormone involved in mineral metabolism and bone growth. Its most dramatic effect is to facilitate intestinal absorption of calcium, although it also stimulates absorption of phosphate and magnesium ions. In the absence of Vitamin D, dietary calcium is not absorbed at all efficiently. Vitamin D stimulates the expression of a number of proteins involved in transporting calcium from the lumen of the intestine, across the epithelial cells and into blood. The best-studied of these calcium transporters is calbindin, an intracellular protein that ferries calcium across the intestinal epithelial cell.
Numerous effects of Vitamin D on bone have been demonstrated. As a transcriptional regulator of bone matrix proteins, it induces the expression of osteocalcin and suppresses synthesis of type I collagen. In cell cultures, Vitamin D stimulates differentiation of osteoclasts. However, studies of humans and animals with Vitamin D deficiency or mutations in the Vitamin D receptor suggest that these effects are perhaps not of major physiologic importance, and that the crutial effect of Vitamin D on bone is to provide the proper balance of calcium and phosphorus to support mineralization.
It turns out that Vitamin D receptors are present in most if not all cells in the body. Additionally, experiments using cultured cells have demonstrated that Vitamin D has potent effects on the growth and differentiation of many types of cells. These findings suggest that Vitamin D has physiologic effects much broader that a role in mineral homeostasis and bone function. This is an active area of research and a much better understanding of this area will likely be available in the near future.
Causes:
- Rickets caused by a deficiency of calcium or vitamin D3 in the diet.
- An imbalance in the calcium to phosphorus ratio in the diet will also result in abnormal bone development and high phosphorus levels in the diet even with normal calcium levels can result in bone disease.
- Commercially formulated diets not scientifically balanced for protein, energy, vitamin and mineral content and other essential ingredients.
- Diets not formulated for particular species and specific ages of bird as the dietary requirements for the bird will change as it grows and develops.
- Home-formulated diets including the feeding of whole grains or scratch grain diets are generally poorly balanced, particularly in the amount of calcium and essential vitamins such as Vitamin D3 or Vitamin A.
- Rickets caused by phosphorus deficiency may be precipitated by force feeding too much calcium even though the ration would otherwise be adequate in phosphorus and vitamin D3.
- Although rickets can occur because of phosphorus deficiency, most outbreaks are the result of inadequate of vitamin D3. Sometimes vitamin D2 erroneously fed to poultry instead of vitamin D3.
- Mycotoxins in feed, especially those produced by Fusarium mould are associated with rickets due to toxic effects on the liver and kidneys. Both of these organs are required to convert Vitamin D3 into active forms required for calcium absorption.
- Diet high in saturated fats such as tallow which bind with calcium in the gastrointestinal tract to form soaps. Such undigested fat reduces the availability of Vitamin D.
- Rancid fat used in feed may cause enteritis and may also destroy available vitamin D3.
- The stability of nutrients and Vitamin D3 may be detoriated by longer storage of time i.e. more than 10 days especially during summer.
- Calcium deficiency develops quickly if newly hatched chicks do not receive an adequate supply. Newly hatch chicks have minimal stores of calcium.
- Enteric diseases.
- Chickens have malabsorption syndrome or infectious stunting may develop rickets even though the ration contains adequate levels of phosphorus and vitamin D3. Failure to absorb and /or utilize nutrients in the ration is considered to be secondary to other causes.
Symptoms:
- Lameness.
- Hock swelling.
- Soft bones and beak.
- Stiff gait.
- Poor growth.
- Birds rest squatting position.
- Reduction in bodyweight.
Diagnosis:
- In young broilers, their age, signs, and lesions are all usefully in diagnosis.
- Softening of beak and beading ribs are almost pathognomonic.
- Carefull calculation of the calcium, phospjorus and vitamin D3 content of ration may reveal that it is deficient or imbalanced.
- Chemical analysis of ration for minerals and Vitamin D3 can be done but it is expensive and time consuming.
Post-mortem lesions:
- Metarsal (shank) bone do not snap crisply when broken but rubbery.
- Bones soft and rubbery and can be bend or flexed easily.
- Epiphyses of long bones enlarged.
- Beading and fracture of ribs.
- Growth plates widened and disorganized.
- Beading of the ribs, most noticeable at their junction with the spinal column.
- Ribs thickened and tend to bend that the thorax is flattened laterally.
- Folding fractures of the long bones and the ribs.
- Parathyroid glands enlarged.

Photo 1: Group of young broiler chicks with rickets. All of these birds are alive but refuse to stand and walk because of the painful changes in the bones

Photo 2: Rubbery Bone

Photo 3: Rubbery Beak
Disease State
The skeleton of young animals grows extremely quickly. Calcium and phosphorus are essential minerals that are critical for proper bone growth and bone strength. The absorption of these minerals and the ability to incorporate them into the growing skeleton is dependent on the availability of Vitamin D3. If either of these nutrients are lacking in the diet, the skeleton will not mineralize properly and the bone strength will be affected. As the bird gains in weight, the soft, poorly mineralized and rubbery bones bend and twist easily. These lesions are painful and the birds are lame and reluctant to walk. Because of the pain and physical deformities the birds have difficulty reaching the feed and water and will lose body condition and eventually die if not treated.
Treatment
Treatment involves:
- Correcting the diet as soon as possible before the bone deformities become too severe to be reversed.
- Adjust the ration to fit the age and performance level of flock. If ration has been deficient in vitamin D3, give Calcium with vitamin D3 preparations like Calcicare or Merical or Solucal three times the usual amount for a period of 1-2 weeks. (Remember, birds can only utilize vitamin D3 not other forms of vitamin D packaged for mammals).
- Capsule Evion - 1 cap for 50 kg body weight.
- Vitamin AD3EC and B-complex through drinking water.
- Along with this Antitox plus or Toxinot should be given.
- Placing birds on a commercial diet designed for that age and species of bird
- Supplementing the feed with calcium for example top-dressing the feed with dicalcium/phosphate or shell grit etc.
- It is generally safe to assume that if the birds are developing rickets on a home-formulated diet, then they likely have other vitamin/mineral dietary problems as well, and so supplementation with multi-vitamin mineral packs may be helpful.
- Proper diets are critical to raising healthy birds. Resist the temptation to buy cheap scratch grains and whole corn. Your investment in properly formulated and well balanced diets will pay dividends in good growth and healthy birds.
Control
- Feed a balanced ration with a adequate calcium, phosphorus and vitamin D3. Chemical antioxidants (santoquin, ethoxyquin,BHT) can be added to help preserve the vitamin D3. Rations should be carefully compounded to fit the age, purpose and performance of the flocks.
- Provide oyster shell or course limestone free choice as a supplemental source of calcium.
Related topics:
Authors:

Suman Hatchery Ltd.
Recommend
Comment
Share

29 de noviembre de 2011
Dear Doc,
Mr. Nitin and myself till awaiting for your feedback.
Please do the needful and update us.
Regards,
Dr. Jaydip
Recommend
Reply

28 de noviembre de 2011
Dear Dr. This article & information has been very useful.
Recommend
Reply
23 de octubre de 2011
Dear dr,
Good article and it gives more information regarding VitD3
Recommend
Reply

22 de octubre de 2011
IT IS INDEED A WONDER FUL ARTICLE EXPLAINING THE DEATAILED ANALYSIS OF DISORDERS ,AND DEFICIENCIES.
PLS GUIDE IF BONE MEAL OR DCP IS MORE EFFICACOIUS IN BROILER RATION.
Recommend
Reply

21 de octubre de 2011
It seems to be more useful to deal with relationships between rickets and other metabolic diseases derived from high genetic potential for management of fast growing flocks.
Recommend
Reply
21 de octubre de 2011
Dear Doc,
Thanks for such a wonderful presentation.
Requesting you to update the information on the line of treatment concerned with generic name of drugs Viz. Vit D3, Calcium, Phosphorus along with optimum doses required per kg body weight in cases of respective deficiency disorders.
Regards,
Dr Jaydip
Recommend
Reply

20 de octubre de 2011
Sometimes we overlook metabolic disorders. This article will help everyone to be conscious about metabolic disorders. Thanks a lot for elaborate presentation...
Recommend
Reply

20 de octubre de 2011
A good informative article especially for beginners in production jobs.
Recommend
Reply


20 de octubre de 2011
Excellent article and nice elabortation of technical matters.
Recommend
Reply

20 de octubre de 2011
Dear Dr,
The article is good, Thanks for giving the details about Vitamin D3 function
Regards,
Neethiraja
Recommend
Reply

Would you like to discuss another topic? Create a new post to engage with experts in the community.
Featured users in Poultry Industry

Shivaram Rao
Pilgrim´s
PhD Director Principal de Nutrición y Servicios Técnicos de Pilgrim’s Pride Corporation
United States
United States





